
Judith
About Judith
Posts by Judith :
Article about Dr. Simon in 168 Ora, in Hungarian. July, 2018.
This is an exclusive interview with Dr. Judith Simon, taken by a well renowned Hungarian Magazine. Her diligence is unparalleled. Her will to help the people suffering in Ghana is unmatched. In this interview, she talks about all her future goals and achievements so far.
Blind School Blog Pt 1: Visit to the blind school in Wa
October 2014
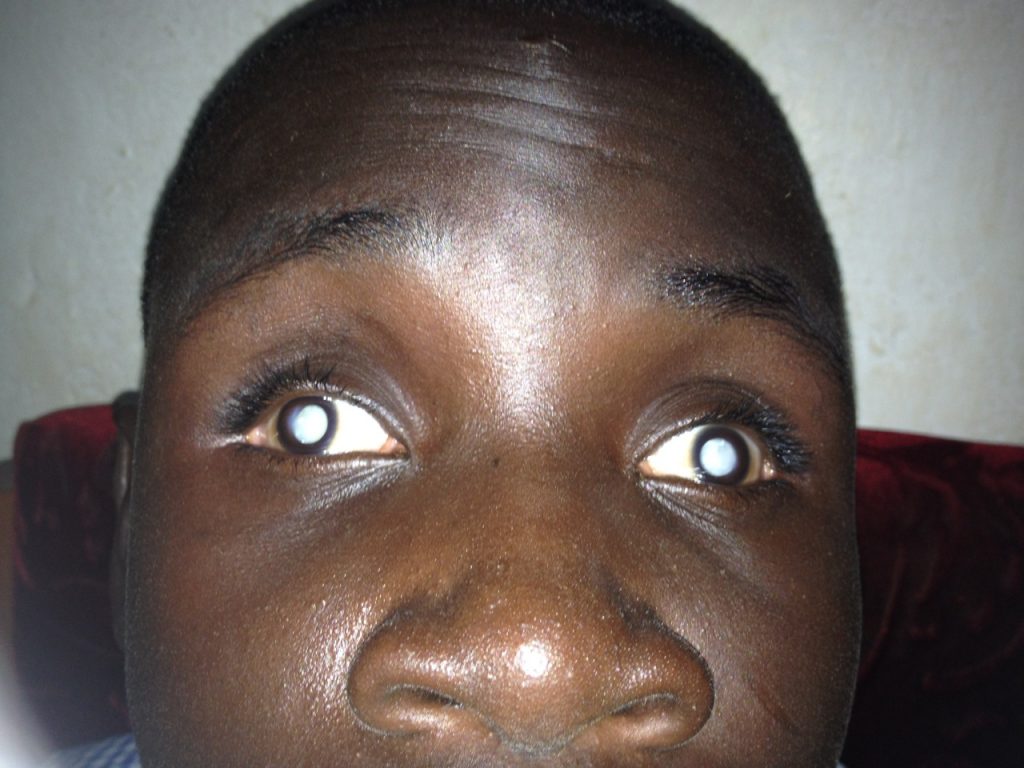
A few months ago I heard from a colleague that upon visiting the blind school in South Ghana he noticed that quite a few children could be helped by simple cataract surgery. There are only two blind schools in Ghana, one of them in Wa, “close” to Tamale. So I decided to organize a trip there to see if there are any children who could be helped by cataract surgery, glasses or by other means. I have been an ophthalmologist for 26 years and I have never been to a blind school, so this seemed like a good opportunity. I also thought of writing an article about the blind school to the Ghana medical journal. So this is the first of my blog series of visit to the Wa Methodist school for the blind.
I recruited my two favorite optometrists, Dr Collins and dr Nicholas, whom I have been working with for over a year. Wa is the regional capital of the most deprived region of Ghana, the Upper West. It has 100 000 inhabitants and only one traffic light. It is 5 hours from Tamale by private car, much longer with public transportation. We requested a car from the hospital, as I did not feel like sitting in a tro-tro with someone’s fat thigh pushing on my side for 7-8 hours. After about twenty phone-calls, e-mails, snail-mail and several personal visits, the transport has been approved. I turned out to be a large bus taking nursing students to the funeral of one of their classmates to a village close to Wa. It is a custom in Ghana that hundreds of people attend funerals and they go to extremes, might travel even for days for this. For Westerners it does not make sense but it is a way for them to show their compassion and solidarity. When I asked what happened to the young man who “passed” (Not “passed away” as we say it), the answer was the standard “he fell sick and died. “ I do not think I have ever heard any other explanation for death here, except if it was an accident.
The bus arrived to our hospital in Tamale around 1pm, about 1/3 full. I was happy we’ll have so much space, but it was too early to rejoice. We toured around Tamale for about 1 ½ more hours to collect more students until the bus was totally full. Then we waited another 30 min for just one person, sitting in the heat, sweating profusely. This would have been inconceivable in any Western country. The patience of Ghanaians is unbelievable. Finally we left and arrived a mere 6 hours later to Wa.
The blind school was established in 1958 by the Methodist Church but now is run mainly by the government. There are 220 students and 72 staff, half of them teachers. The students learn the same curriculum as the regular students, just in Braille, and in addition some receives vocational training, like basket weaving. The students speak many different languages, lots of them do not speak English and some have no common language with the staff. This, in addition to their mental and physical disabilities makes teaching them a real challenge. In spite of this, some still continue to university and became teachers themselves.
We got to our lodging and started work the next morning. We had preprinted sheets, and the teachers were filling in the names, the vision and the history. About 15 students filed into the room, were examined and sent out, then the next batch came. It was very interesting that most children walked around as if they were seeing perfectly well, even the totally blind ones. In the beginning the screening went slowly, but by early afternoon we improved on the system and speeded up. At the end of the first day we examined 150 students and identified 15 who could be helped.
At night we were returning from town when we saw a man walking home. We said hello and he told us he was one of the teachers there. From the way he moved I was pretty sure he was sighted but then I noticed he had dark glasses on. He said he was completely blind, his eyes were removed as a child. He attended this school and later he returned as a teacher of math and moral studies. We asked him how he could get around being blind, he laughed and said he just knew the place. When we got near to his house, he turned and walked home. He could hear his radio and that is how he knew where to turn. Later I left our lodging to take some leftover food to the fridge of the main building, which was about 3 min walk, and I got totally lost as the dark was disorienting even that I had a light. I felt like an idiot and was hoping I would not need to ask a blind person for directions. (Finally I found my way.)
The next day we continued the screening and examined another 70 students, 5 of whom could be helped. About ¼th of the students were completely blind, the rest of them partially sighted. About half were born blind, the others lost their sight in childhood. We saw all kinds of amazing pathology – genetic diseases, accidents, eye perforations from measles, all kinds of cataracts and botched surgeries, albinos, etc. Probably the sight of about half of the children could have been saved in the Western world.
The children in the blind school were extremely well behaved, calm and cooperative. They seemed to be happy and satisfied, almost serene. According to the teachers, they do not fight. They were walking around the campus as if they were sighted, the partially sighted ones holding the hand of the totally blind. The teachers of the blind school seemed dedicated and they knew all the children personally. They were mainly middle-aged women and they complained a bit about the lack of resources and difficult working environment. I asked them why they do not try to solicit help from the Western World, or even from Ghana, but then I remembered that they are computer illiterate and inundated with work. I tried to get the e-mail or even phone number of some staff who are young, motivated and have e-mail, thinking that I’d try to link them up with a Western organization, but all I got was two names and a promise that they’d text it to me later. It was a maddening thought to remember all
We asked the teachers if the families come and visit, and they said no, never, not any of them. The reason they gave was mainly poverty, and also that “the families do not want trouble”. During

After we finished work we asked to see the lunchroom, the sleeping quarters and the classrooms of the school. One of the large halls burned down a few months ago so they were using the same hall for lunch and assemblies. A bell signaled the time for lunch, but the students were already gathering in front of the hall about 10 minutes early, even though they did not have watches. Inside there were simple wooden tables and benches, and a blind girl was carrying a bench nearly hitting a few others, not noticing it was broken. There were metal dishes and plates, and the children were served food by their “house mothers”. These ladies take care of all tasks a mother usually has, and there were 5 for the 220 students in the whole blind school. They must be exceptional women. The children got rice and an egg. They hardly ever eat meet and never fruit, as these are too expensive. The scene reminded me of a prison canteen, though the students were calm and patient. There was a brief silence as they stood up and prayed before the meal. It was
Blind school blog Pt 2: Exam day in Tamale Teaching Hospital
30 January 2015
Today 16 children with 4 teachers came from the Blind School in Wa for exam to our hospital. I raised some funds for their transportation so they took their own bus. They arrived around 1pm. We started the exam right away while a teacher got their folders. They were extremely cooperative and respectful – very easy patients. Out of the 11 possible surgical candidates we identified 9, and 2 could be helped by glasses. A student got an injection for a blind, painful eye and a prosthesis to the other eye which was removed earlier because of pain. We took them to have an ultrasound and lab-work for future anesthesia. They marched around the hospital in their uniform bravely, hardly letting us hold their hands.
I examined the teachers too and one of them, Abdul-Salaam was found to have diabetes, hypertension and glaucoma, all of which he was unaware of.

They brought their food with them and after the exam, they sat down to eat – just rice with sauce. Then they took off to make the 5-hour journey back home, unfortunately in the dark. It is not advisable in developing countries to drive after sunset, as the chance of an accident is much higher. Fortunately, they arrived unharmed.

Blind school blog Pt 3: First surgery day
19 February 2015
Yesterday 3 blind children came with one of their teachers, Abdul-Salaam from the Wa Blind School for surgery to our hospital. They took public transportation: tro-tro and shared taxi, as there is no money for them to take their own car. They arrived around 5pm, a bit exhausted, thirsty and hungry. We gave them water, got their folders in order and took them up to the hospital floor for admission. The nurse assured us that they will get dinner and breakfast. One boy who is 12 years old needed general anesthesia, so we repeatedly told him not to have breakfast. I checked the teacher’s eye pressures who has glaucoma and then we went home, as he was staying with me.
We had dinner together and he told me a few interesting stories: The attorney general of Ghana is his brother. He is blind and graduated from the Blind School in Wa before going to university. He became blind from measles, which can cause corneal perforation in malnourished children. This is how Abdul-Salaam became interested in working with the blind. He taught himself Braille and to translate from English to Braille. He is one of the few experts in this in Ghana, and because of this, he is held in very high esteem by the blind community, as he saves a tremendous amount of money to the government with his expertise. The Minister of Chieftaincy, Henry Siedu Daanaa, who is also blind and graduated from the Wa Blind School is his brother-in-law. He is a good friend to his blind brother and that is how he met his sister. He talked about the difficult conditions in the school: The government has not been paying them for over 2 months and they owe a lot of money to the food suppliers, some of whom stopped delivering food. They cannot pay the trash collection fee either so the trash is just standing there.

Next morning we went to the hospital together. The children were brought down from the ward. We asked the 12 years old if he had breakfast, he said no. It came out in the afternoon that neither the other two children ate, and they did not have dinner either the night before. (But they did not complain at all.) The hospital has no money to buy even food now. I wish the nurse had told us this.

The surgeries went very well even though they were not easy. The scrub nurse was a student who had no idea what to do, and I had to train him while I was struggling with the eyes. But I got used to this over the past two years, better to keep quiet and try to manage than to make a scene. After finishing the children we operated on an old man with a cataract, the other eye blind, a very difficult case; then a young glaucoma patient, also blind in his other eye. He was also from Wa, so I wanted him to take the children with him, but he is also taking public transport the next day, so he will join Abdul-Salaam.
After finishing the surgeries we tidied up the OR, saw a few waiting patients, bought the children food, and left. I am so much hoping they will see at least a little better tomorrow!
Blind school blog Pt 4: Second surgery day
February 26 2015
On Wednesday, the 3 teenagers operated on last week returned for follow-up from Wa. All 3 claimed to see better. Mohammed, age 17, who had vision of light perception, improved to count fingers 2 meters, but he has an extremely small eye (called microphthalmos) so we did not expect that much more improvement. Bayiiri, age 12, had the same improvement in both of his eyes. He has been blind since birth, from cataracts, so his prognosis is not too good, as his brain never learned how to see. But he was very happy and his teacher told me he saw him reading the Bible alone! I was a bit sceptical, as he knows only Braille, but the teacher assured me all blind children still know how letters look like.
The third youth, Richard (age 22) could see nearly normally, he could read 2/3 of the distance eye chart and also medium-sized letters! He had been blind for 12 years! He told me the story of his blindness: (A quite common story in the blind school). When he was 10 years old, he went to fetch water, and he experienced a severe headache. He returned home and complained to his mother, who admonished him. Later he became very sick, developed a fever, was taken to the hospital, and when he was discharged, he could see just minimally. Later he was taken to a different hospital, got eye-drops, but his sight did not improve. Then he was taken to a third hospital, he received treatment, after which his remaining vision was also lost. He started to attend the Blind School at age 13. Now he can walk around alone, can read and can do everything a sighted person can do! He was helping out a lot with the other blind children who came for surgery. He was very excited about returning to his village sighted. I wish I had the time to go with him to see his family’s reaction. (Though people in developing countries are quite stoic in general, over the years I saw only a handful of patients who showed their emotions upon regaining their sight.)
I asked Richard about his plans. He said he would probably finish school in Wa, as he is in his last year. The teacher said he can be “mainstreamed” now, meaning he can go to regular school. One of my fears upon embarking on this project was that children will not want to see: They have a safe place in Wa, it is free, they are getting fed (even if it is only rice), get clothing (even if it is torn), have a bed, they go to school, have caring teachers, they have friends, a community. They also receive vocational training. Life is probably much worse in the village even if someone is sighted: No schooling, hard farm work, scarce food, no hope of ever leaving from there, of ever getting a profession…. Well, we will see what happens long-term.
Thursday we did surgery on 3 more children, all three of them bilaterally blind. They were from age 9-12, so they needed general anaesthesia. We also operated on Richard’s other eye – initially I deemed his prognosis so poor that I suggested to operate only on one eye first. Thank God, I was wrong!
The surgeries went well, though we had the usual problems: Patients arrive half hour late from floor, no anesthetist, (finally, after extensive begging one came) no oxygen, no anaesthetic drugs, no gloves. The power went out during surgery, no one to turn generator on, so I had to break sterility and run outside to do it…but by now I am used to these difficulties and they do not phase me the least bit.


Rosemary, the teacher who came with the children, was excellent, calmed them, fed and bathed them, and took really good care of them. David, a 10-year-old cried horribly for over an hour after surgery, wanted to tear his patches off, it was heartbreaking to listen to it. Finally, we gave him some sedatives. At the end of the day everyone left, the children were taken up to the hospital ward. As I am leaving the clinic (I am always the last one to leave), I discover one of our patients, 12-year-old Lovia, sleeping peacefully on a bed in front of the OR, with both eyes padded. She did not wake up from anesthesia yet. This is Ghanaian postop care – just leave the patient alone till she wakes. I imagined how it would be – waking up totally blind, with two eye pads, alone, not knowing where one is….luckily she did not wake. A little while later the teacher and the house officer came to pick her up.


Next day we saw the 4 postops, gave them eye drops and instructions. It was too early to see any improvement, but I could see the back of their eyes, which is a good sign, it means eventually they should be able to see. They returned to Wa with the noon bus, getting there around 7 pm. The last batch will come next week.
Blind school blog Pt 5: Third surgery day
March 5 2015
On Wednesday, the three children operated on last week returned for follow-up from Wa. All three claimed to see better, be “very happy” and also function better according to the teachers. One has to be careful though with what patients and family members say about improvement: It is not accepted culturally here to displease someone who made an effort to do good to you. Over many years the only feedback I received indirectly about ANY patient from doctors and nurses who did the follow-up was “Everybody’s fine”. No one ever did poorly, which is of course not possible. In the clinic, when we ask patients if they see improvement after surgery, even those who do not read any more on the chart than before claim they see better. It is just politeness, and also Africans frequently tell you what you want to hear, not the truth. They also do not complain much and are eager to please.
Lovia, the 12-year-old girl who has been blind since birth saw the same objectively, but looked more animated. Unfortunately we did not have time to assess her thoroughly, but she still could not walk around unaided. David, who had cataract surgery before, but shortly after an inflammatory membrane blocked his vision again, could move around alone now and could obviously see the near chart as he was pointing at the Es on it. But we could not explain him the E-game (show which way the E goes) as he believed it was still Braille and kept on touching the letters to feel them. Prosper saw amazingly well, he could read about half of the near chart.
The last three children for surgery were all teenagers, old enough to withstand local anaesthesia, even if it was in both eyes. It is amazing how brave African children are – they are used to pain since an early age, know it is part of life, and their pain-threshold is unbelievably high. They also do not get too worried or nervous about procedures, they are extremely brave and also stoic.
One of the teachers, Abdul-Salaam returned with the three postops on Thursday, and the other three had surgery. The surgeries went well, and I was also a bit less nervous as I got some experience with the previous cases.
Rose-Mary stayed with them till the evening, fed them, and bathed them. She returned to my house at 8pm, we had dinner together and talked a lot. I am so happy I got to know her– she is an exceptionally caring person, sweet, honest, and unpretentious.
We saw the postops on Friday, snapped some photos (as they say it in Ghana) then they returned to Wa with the tro-tro around noon. I called them a few times since to see how they are, and they are all “fine”! I’ll go and see them in 3 weeks, but this time I am going to go to Wa, it is easier than to have all 9 of them come to Tamale again.
Blind school blog Pt 6: Follow-up visit to the blind school in Wa
March 27-29 2015
Three weeks after the last 3 children were operated on, we decided to go to Wa to see them. I took my engineer friend, Mashood, who is from a village close to Wa. He could help with the exams and also with translation, as he speaks Wale, the local language.
We took public transport to save money, but this is a bit uncomfortable in Africa. We just missed the tro-tro so we had to wait over 2 hours for the next one. It took us 6 hours to pass the 300 km route. I started to watch a French movie in the dark on my computer to pass the time, “Immoral Tales”. It was basically soft porn disguised as an art movie. After a while I noticed that half of the bus was watching it with me, so I though I better stop. We finally arrived at midnight, without bus-breakdown or accident. One of the teachers, Abdul-Salaam was waiting for us at the station. Next morning we started to work – unpacked the instruments, put the eye-chart on the wall and called for the children. We got an air-conditioned office to use, which was a huge favor!
I just recently finished reading an extremely interesting book: “Crashing Through”, a non-fiction account of an American man who got blinded at age 3 and regained his vision at age 30. As he had visual deprivation for so long, the vision he regained was not normal. He could see motion, objects, colors but he could not recognize faces, could not read (even that he could see the letters separately) or drive, even years after the surgery. He also found it extremely overwhelming to navigate with vision, as it was hard work for him to see – similar to trying to speak a foreign language that one learned as an adult. At one point he regretted ever having the surgery. I also read similar reports about others in the same situation. I got very worried towards the end of the book and thought to myself: “What have I done???” I also remembered one of the favorite phrases of my Mother: “The road to hell is paved with good intentions.” So I was understandably very anxious about the visit.
The children filed in in groups of three. All of them could walk unaided now, except for Lovia. The 12 years old girl had the worst prognosis, as she has been blind from birth. Objectively her vision still remained hand-motion, but she reported to be able to see significantly better. The back of her eyes looked perfectly normal, which made my heart ache, as it means that if her cataracts were removed at an early age, now she could see very well. She can distinguish colors now (probably she learned them during the month since her surgery) and also shapes, she recognizes objects like book, computer, etc and she sees people standing around her. She can even see a picture now and recognize a human face on it.
Mubarak, 20 years old had tiny eyes (called microphthalmos) and already had surgery in one eye. We operated on the other eye, hoping it will get at least as “good” as the first one. He did not improve (the operated eye was even smaller and more abnormal looking than the other) but he said this eye is now helping him to see better in the other eye. I do not have any explanation for this, unless he just said it to make us happy.
Richard, the 22 year old man had the best result: Now he could see 20/40 which is basically normal vision. The interesting thing was that he kept on complaining about his other eye, which improved only minimally. When asked about his future plans, he said he wanted to go to university and become a teacher, but he wanted to continue to study in Braille. (In spite of Ghana being quite poor, it can accommodate blind students at universities.) I made him read, and he knew most of the letters but had problems connecting them. He could read about half of the words though, so I think he will be able to read fluently soon, as he lost his vision when he was 10.
Mayiiri, who had his eyes very shaky (called nystagmus) and turning inside severely, could see a large E from about 3 meters. (Before he could see only hand motion.) He could walk alone now, could see colours, objects and faces. He is mischievous and terrorizes the other children, so they expressed their hope that he would soon improve enough to be able to leave to school!
The rest of the children also improved, two more enough that they will probably be able to return to normal school. We will make another trip to

THE TRIP HOME
We were waiting for over three hours at the roadside in Mashood’s village for the bus. Finally we received a call from Abdul-Salaam that the bus left Wa. In Africa usually there are no scheduled buses, they just leave as soon as they get full, which could take several hours. The reason of it is poverty; drivers are not able to charge more for tickets to cover the expenses of empty seats, as people cannot afford to pay. Usually there are also plastic stools in the center in between seats for people to sit on, to make sure the company makes more “profit” as the profit margin is minimal. For example. a 6-hour bus journey costs less than 6$. People with means travel by car, not by public transport.
The bus arrived and stopped, though there was no bus stop. (We waved as we were told it would be blue.) It was a nice large bus, but Mashood noted right away it did not look “good” to him. He has tremendous experience in Ghanaian public transport as he travels to Kofurudia each weekend to school and back – a 14 hour journey one-way. I soon saw what he meant – the driver’s aid kept on filling the coolant tank with water about every 20 minutes. (The engine was up front, next to the driver). After about an hour the engine started to rattle loudly, and shortly after the bus stopped at the roadside. “The engine got spoiled as there was no oil in it” – declared Mashood as he could make the diagnosis just by the sound of it. I was hoping he was wrong, but he was not. The driver disappeared at a roadside house to make a call for about half hour – I guess he was afraid of being lynched. Then he told us another bus will come soon to pick us up. I thought this to be highly unlikely as African companies rarely have a backup bus to replace the broken down ones. In an hour a large truck arrived and we all climbed on to the open plateau. People were standing or sitting down, some sat on the top of the iron bars covering the sides. I just lied down on the plateau (a bit dirty and hard), put my head on my backpack and listened to a podcast from NPR. It was now late afternoon, the heat subsided, fresh and pleasantly warm wind was blowing on us, the landscape was beautiful, the smell of unspoiled nature penetrated the air…. Then it got dark and I was staring at the moon and the stars. I felt happy and free. Mashood complained about the terrible journey, but I told him it beats a trip in an air-conditioned car. I asked him to imagine how boring my life was in the US if I enjoy an experience even like this!
After an hour and a half we arrived to Damongo, where a small tro-tro was waiting for us. It obviously could not accommodate all the passengers of the original bus. We fought for our lives and succeeded to push on, though I was half sitting in the lap of another man. (Like all other people.) So we left in the dark and a mere 3 hours later we arrived to Tamale. I am not sure though if I’ll risk another public transport journey in Ghana in the near future, we will see!
Blind school blog Pt 7: 2 year follow-up visit to the blind school in Wa
15 February 2017.
We just had 8 children come from the blind school for follow-up, so we paid for their trip and food. We operated on them 2 years ago (for congenital cataract) and 2 already left the blind-school! One more could also leave, and all of them improved a lot in their functioning. It was very heart-warming to see them again. Even the way they walked into the exam room, they did not seem to be blind any more, as they could come in and sit down in a chair unassisted. I should write it up as an article but I have no time for it.
We tried to asses their visual function with some questions, as the visual acuity usually does not improve at all, or only minimally unless the cataract is operated on before 3 months of age. It is because of the development of a lazy eye. (The medical name for it is amblyopia, meaning the brain does not learn how to see as it did not get any visual input for a while).
The children gave the following answers :
« Now I can see colors »
« Now I can walk around without help »
« Now I can count money « (i.e, See the amount from the color of the bills.)
« When I go home, I can sweep the house »
« When I go home, I can tell the difference between grass and maize » (I.e, I can weed.)
There was one more blind girl with them with bilateral cataracts, who initially did not agree to the surgery, but now that she witnessed the others seeing better also wanted to undergo the operation. We performed it (only on one eye for now) and we are hoping she will also improve and agree to the surgery of the second eye.
Mission Diary 2014, Zabzugu, Ghana
January 25, 2014
It is 2:50 AM and I am at 36,000 feet with an airspeed of 581 miles per hour. The Captain says there are strong winds and my thoughts drift to the beloved character of Mary Poppins. And like her, I too am being carried to a place desperately in need of organization, discipline and love, though I am not headed to 22 Cherry Tree Lane. My east wind is blowing me to Ghana.
What is it that inspires philanthropy?
What life experiences propel one’s desire to create a greater global good? I think about these questions as I stare out the window into the darkness, for here I am embarking on another Right To Sight medical mission.
Mary Poppins used a spoonful of sugar to make the medicine go down. If only it were that easy! The recipe fashioned for our medical outreach was quite a bit more involved and in need of many ingredients. In the end, however, it went sweetly down as if it too were sugar coated.
Recipe For A Right to Sight Outreach
Ingredients:
2 cups enthusiasm
2 cups determination
1 cup commitment
large handful perseverance
1 bunch motivation
pinch of frustration
2 heaping tablespoons humility
diligence to taste
sprinkle with patience as needed
Directions:
Mix together enthusiasm and determination. Add in commitment. In separate bowl, beat together a large handful of perseverance and bunch of motivation. Blend into first mixture. Season with patience as needed and simmer with diligence. Add in a pinch of frustration and 2 tablespoons humility. Cover with cloth to keep out dust and mosquitoes. Let mixture bake under the hot Ghana sun.
Serve with education, good intentions, and friendship.
Should keep fresh for one year without refrigeration.
Each of the above ingredients were necessary to make the outreach a success and yet none could stand alone, for it was the sum of all the parts that created the real magic.
Dr. Judith Simon led our team through her hard work, dedication and commitment. She attempted for months to pull together resources, contacts and organizations as she laid the ground work for outreach approval in the Northern region. It was a daunting task to piece the mission together and coordinate the decisions from the many personalities needed for our approval…..Village Chiefs, hospital administrators, medical directors, district mayors, Tamale Teaching Hospital staff officials, Swiss Red Cross, Ghana Red Cross, interns, students, nurses, and friends. Long hours, inconveniences, misinformation, and bureaucratic run-around continually plagued her good intentions. I felt her upbeat attitude beginning to waiver and her faith in accomplishing this mission wearing thin. With no clear answers, I flew to Ghana determined to keep pushing and working towards the outreach approval.
There is an old saying…”sticks in a bundle don’t break”. I would add my fresh perspective and “energico” which I concluded were critically needed. Judith had confided in me that if an outreach were to happen, we probably wouldn’t know until most likely the day before. I may be mistaken, but I sensed the “powers that be” just got tired of us asking and pushing, surprised we had not given up (does a Jersey Girl ever give up??). Then true to her prediction, we received our “go ahead” on a Wednesday night. Within minutes, she contacted a new intern optometrist, Dr. Collins, and extended the invitation to join our outreach. He agreed with enthusiasm and was sent out to the rural community of Zabzugu and Tatale to begin prescreening some 24 hours later. Mr. Razak of the Swiss Red Cross helped coordinate transportation of patients, and Mr. Alidu arranged the meeting with the village Chief at his palace (Kola nuts the traditional gift and a must for formal introductions).
Our team functioned with mutual respect for each other, creating a deep sense of camaraderie. With the help of the Tamale Teaching Hospital eye nurses, Lucianus, Imaculate, and Momed, we packed and loaded supplies from the clinic, hospital operating room, as well as including packing personal and donated supplies. We then traveled some 3 hours to the rural community of Zabzugu. There in the district hospital we unpacked and organized our pre op, post op, and operating room supplies…. gloves, drapes, dilating drops, steroidal drops, instrument sets, blades, microscopes, intraocular lenses, IV fluids, cannulas, syringes, needles, sutures, antibiotics, q-tips, gauze, tape, sanitizer, cautery, basins, autoclave, eye charts, scanners, ophthalmoscopes, flashlights, antiseptic, alcohol, water, and don’t forget the duct tape! The hospital seemed much like a ghost town, with many empty rooms and wards. Though a fine looking facility (though it could have used running water) there are few to no doctors to fill this place (2 ophthalmologists for 2.5 million people in Northern Region). The setting provided the perfect conditions for me to educate the Ghanaese healthcare workers. Sterile technique, infection control, patient processing, skills that enhance the safe delivery of care, and finally compassion…an often overlooked virtue necessary when taking care of the elderly.
It was an awesome outreach with a great learning curve. We accomplished so much in a short amount of time even though frustration and politics clung to our actions. District’s medical directors refused to send prescreened patients to our location because they wanted the notoriety in their own village’s hospital. I must mention it was the owner of the A.B.M. Hotel we stayed at who aided our fledgling efforts by providing a vehicle to help transport those patients stranded in the outlying villages. We did 10’s of surgeries instead of 100’s, yet I am not disappointed.
There is another old saying…”to save one life is to save the world”. It is a miracle to restore someone’s sight and be part of that process. I will never be able to put into words the look of joy you see flood in someone’s eyes the day after surgery when their eye patch is removed. I will never be able to explain the feeling of humility when someone bows to you or kneels at your feet or kisses your hand with pure unadulterated gratitude. I only know that at the exact moment when our eyes meet, we both see something wonderful…for it is not necessarily sight we have, but insight. When you can see past color, race, religion, or culture…when everything disappears from sight except one human helping another, what you are left with is the best vision of all.
Eventually the winds changed and a west wind carried me back home again to New Jersey where I find myself dreaming of another Right To Sight outreach. I wish to personally express my deepest thanks to the 2014 Ghana team. One at a time we really are changing the way the world sees.
Beth Weston Knotts, R.N.
February 2014